Select your region
-
Europe
-
Americas
-
Africa and Middle East
-
Asia Pacific
The BaSICS (Baby Skin Integrity Comparison Survey) study:
Paper 2

698 mothers and babies, 38,390 nappy changes: what did we learn?
Abstract
Background: Several industry funded studies between 2001–2018 have compared the use of a single brand of baby wipes to cleansing with water and either cloth or cotton wool during nappy changes. All of these studies found that wipes were safe and effective from birth. Recommendations from these studies have included the need for brand or formula comparison but to date, no previous study has done this.
Aims: The ‘Baby skin integrity comparison survey’ (BaSICS) study was designed to compare three brands of baby wipes to determine if there was any difference in the incidence of irritant diaper dermatitis (IDD or nappy rash) during the first eight weeks of life.
Methods: Mothers who were allocated to a single brand of nappy but divided into three baby wipe allocation groups, collected and reported survey data on infant skin integrity during one nappy change daily with the use of a user-friendly smartphone application.
Findings: All brands of wipes were acceptable to mothers and safe and effective when cleaning during nappy changes. The brand containing the fewest ingredients showed a clinically significant advantage of fewer incidents of rash than the other two brands.
Conclusion: This study demonstrated that wipe formulation is a significant factor in prevention or reduction of IDD during the first eight weeks of life.
In 2018, a midwifery research group in the North of England was commissioned by a manufacturer of baby wipes to compare three brands of wipes, including their own, to determine whether there was any significant difference between products. The manufacturer’s initial hypothesis that their wipes protected against nappy rash was based on anecdotal evidence.
To ensure lack of bias, good scientific practice and ethical research conduct, they engaged a university based research group to design and implement a prospective experimental study, as defined by Salkind (2010), to conduct a brand comparison with daily use of baby wipes during the first eight weeks of life.
The title of the study is the ‘Baby skin integrity comparison survey’ (BaSICS) study and the location in which the study took place was a major urban district that included outlying suburban and rural areas.
This location was selected as it represented a diverse population in terms of both ethnicity and socioeconomic classification. The aim of the research was to determine whether there was any difference in the incidence of irritant diaper dermatitis (IDD), also known as nappy rash, when different brands of baby wipes were used to cleanse the skin during nappy changes when the brand of nappy was the same across all three arms of the study.
Background
With the advent of disposable nappies and baby wet wipes, nappy area care may seem simple and straightforward. However, there are still unanswered questions about IDD such as why some babies seem more susceptible than others, and whether some brands of products, such as wet wipes, are more effective in preventing soreness and rash than others.
This remains an important question in newborn skincare as a substantial number of infants will display some disruption of skin integrity in the perineum,groin, thighs and buttocks by the age of one week; the severity of skin breakdown increases by week three (Goldman and Lodhi, 2016).
Several studies within the past two decades have examined the problem of infant skin health in relation to methods used to clean the skin during nappy changes. Two important trials (Visscher et al, 2009; Lavender et al, 2012 found that the traditional methods of newborn skin cleansing using water and cloth or cotton wool are no better in maintaining skin integrity and hydration than the use of disposable wipes, while the latter are
preferred by parents for their ease of use and effective cleansing properties. Both of these studies compared water with a single brand of
baby wipes and recommended future brand comparisons.
A study on older infants who were approximately nine months of age at the start also compared the use of water with the use of baby wipes and found wipes to be as safe and effective as water (Garcia
Bartels et al, 2014).
These findings were congruent with those of an earlier study that used a visual assessment of erythema and IDD to compare the use of water with that of a single baby wipe product (Ehretsmann et al, 2001). A more recent systematic review has confirmed the comparable ability of water and wipes to cleanse newborn skin safely and effectively (Cooke et al, 2018). A European roundtable updated recommendations for infant skincare to include the use of baby wipes as an acceptable alternative to cleaning with water at nappy changes (Blume-Petayvi et al, 2016) and
a recent US study confirmed the safety and effectiveness of low-ingredient baby wipes in a nappy rash prevention and treatment protocol for neonatal intensive care units (NICU) (Rogers et al, 2020).
Methods
The active study period covered approximately 18 months once a study protocol had been approved and research staff recruited. During the first
months of the study, the team was engaged with obtaining university, and then national, ethical approval, working together with a commercial IT firm to design and develop a data collection digital application, obtaining research passports for the three research assistants and creating all the necessary documentation to support the study.
This included letters of invitation, consent forms, information sheets and poster advertisements for display in antenatal clinics.
Preliminary work also involved meeting with midwifery managers, researchers and clinical midwives to explain the study and to elicit their support in the recruitment process. The research team worked closely with local NHS trusts and obtained permission to recruit participants in three regional hospitals and associated community antenatal clinics. When all these factors were in place, recruitment began. A power calculation was done to determine the sample size required to detect meaningful statistical differences between the three brands of wipes (Jones et al, 2003). This determined that to detect a 10% difference
in rates of IDD between one brand and another, 166 women would need to be recruited to each study arm. As clinical studies often have quite high dropout rates, with many trials only achieving around 56% of their target population (Walters et al, 2019), the research team planned for an attrition rate of approximately 30%, setting a recruitment target of 700 participants.
Women over the age of 18, pregnant with a singleton fetus, who had no serious medical problems that could affect their baby’s health, were recruited from 34 weeks of pregnancy. Three part-time research assistants were responsible for the initial recruitment, each working in one NHS trust area in order to establish relationships with maternity staff and to create their own case loads of women from
the same geographical area.
One research assistant was a former midwife, another was an experienced research assistant on mother and child projects, and the third was a mature final year psychology student.
Later, when information about the study appeared on university social media pages and in the local press, women began self-referring to the study or using a snowball sampling technique to recruit friends and family members (Lewis-Becket al, 2004).
Women who had obtained information frommaternity groups on social
media platforms or who had seen information posters in local hospitals also referred themselves to the study. As long as potential participants met the inclusion criteria, which included maternity booking with one of three local NHS trusts, they were invited to meet a member of the research team to learn more about the study. If women then wished to participate, they were asked to sign a consent form. In total, 737 women
were enrolled onto the study, with 722 eligible to commence the surveys at the time of their baby’s birth.
A total of 15 women were unable to participate as their babies no longer met the entry criteria at the time of birth, either due to health problems necessitating admission to NICU or prematurity. Retention on the study was very high, with only 24 participants exiting the study prior to completion.
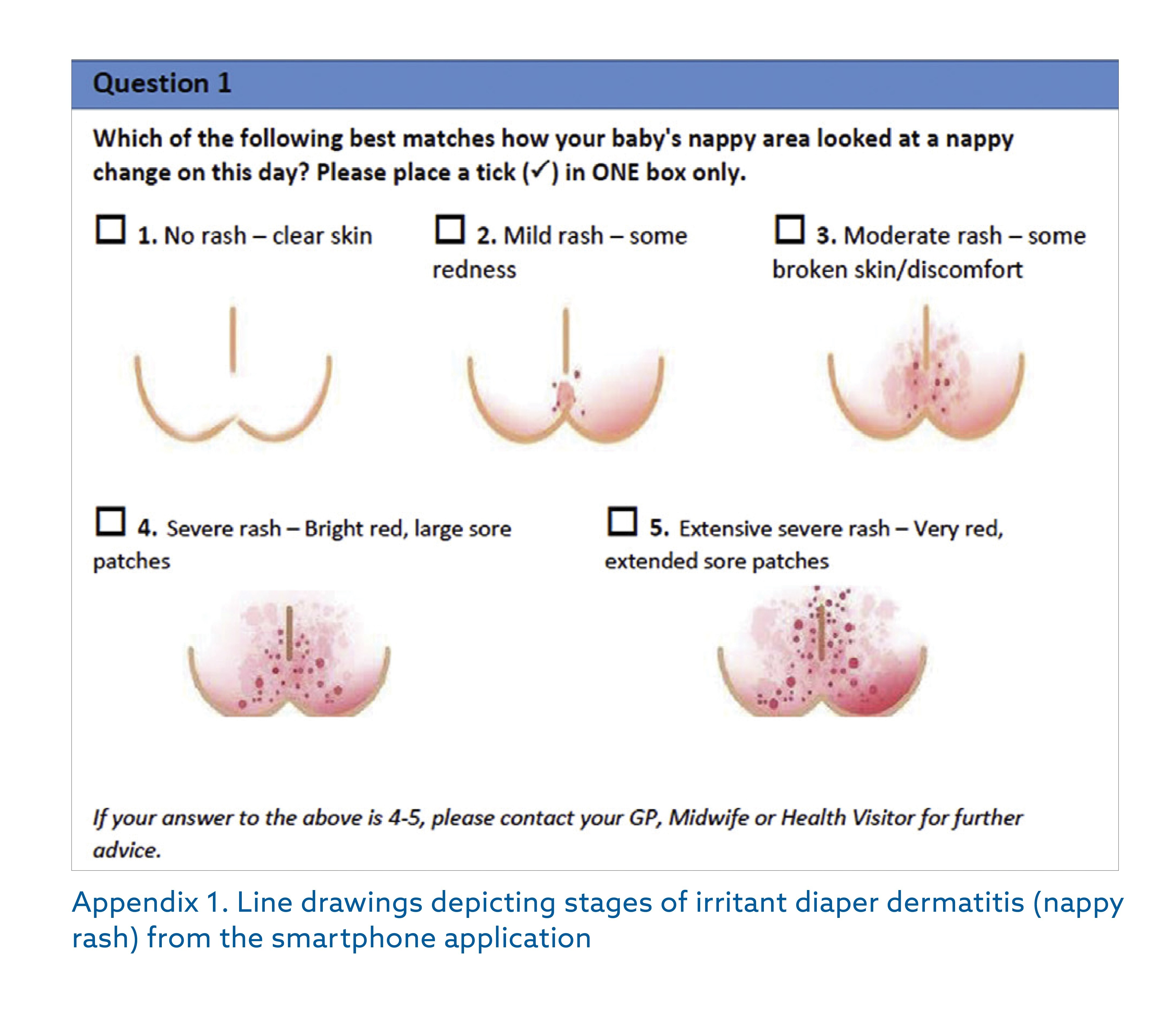
The survey tool was a custom-designed, user-friendly digital phone or web-based application that participants downloaded on signing the consent form. A paper-based survey tool was available for any participant who preferred not to use digital technology (n=3).The survey consisted of four simple questions about the baby’s skin conditionand included a written description and pictorial representation of nappy rash to help mothersdetermine which category most closely matched the appearance of their baby’s bottom (Appendix 1).
Mothers selected a number from one (no rash) to five (severe rash) using a scale created by a neonatal specialist practitioner on the research from the smartphone application advisory board adapted from a previously
validated tool (Buckley Dofitas et al, 2016).
Activation of the application required entering the baby’s birthdate at the time of the first entry; this triggered 55 consecutive days of the same survey questions followed by a longer final survey on day 56 (Appendix 2).
The final survey, adapted from a questionnaire validated in an earlier study by Furber et al (2012), was designed to assist in achieving a broader understanding of the research participants and their experiences. More detailed findings from the final survey will be reported in a
future paper.
Women retained in the study achieved 100% compliance in completing the daily survey, helped by automated reminders sent by text or email. At
the end of the study, 10% of participants were selected randomly and invited to participate in a final qualitative phase of the study.This was
designed to explore their experiences of participation in the study and perceptions about infant skincare in greater depth. Approximately half
of the women approached agreed to be interviewed (n=36). The methods and findings of the qualitative component of the study will be reported in a future paper.
Following enrollment onto the study, participants received a ‘starter pack’ of nappies and wipes for use from the birth of their baby. All participants
received the same brand of disposable nappies and one of three brands of baby wipes determined by a process of blocked randomisation to reduce any potential bias and achieve balance in the distribution of participants to the three different study arms (Efird, 2010).
Activation of the survey tool triggered fortnightly delivery of nappies and wipes to each participant by a local storage and courier firm. In total, each participant received nine weeks’ worth of nappies and wipes. Although the researchers doing the statistical analysis were blind as to which participants had been assigned to which brand of wipe, it was not
possible to blind participants to the brand they received. This would
have necessitated re-packaging all wipes in plain wrappers and this
could have raised questions about compromise to the quality of the
wipes. All three brands of baby wipes were common brands advertised
as being gentle enough for newborn babies.They were identified in the
study simply as Brands 1, 2 and 3.
Quantitative analysis of the daily survey data and the final ‘day 56’
survey were done using SPSS and Stata Univariate comparisons
between the three brands. ANOVA, Chi Square and Kruskall Wallis tests
were used to compare characteristics of the sample. Day 56 survey
results will be reported in a future paper
Results
In total, 698 mother and baby pairs completed eight weeks of daily
surveys. Findings from the whole sample showed an incidence of IDD
during the first eight weeks of life of 24.6%, which is similar to other
reported studies (Philipp el at, 1997; Ravanfare et al, 2012). However,
as methods of assessment varied between studies, it is not possible to
make any direct comparisons. The factor that makes the BaSICS study
unique is that it compared three different brands of baby wipes, all with
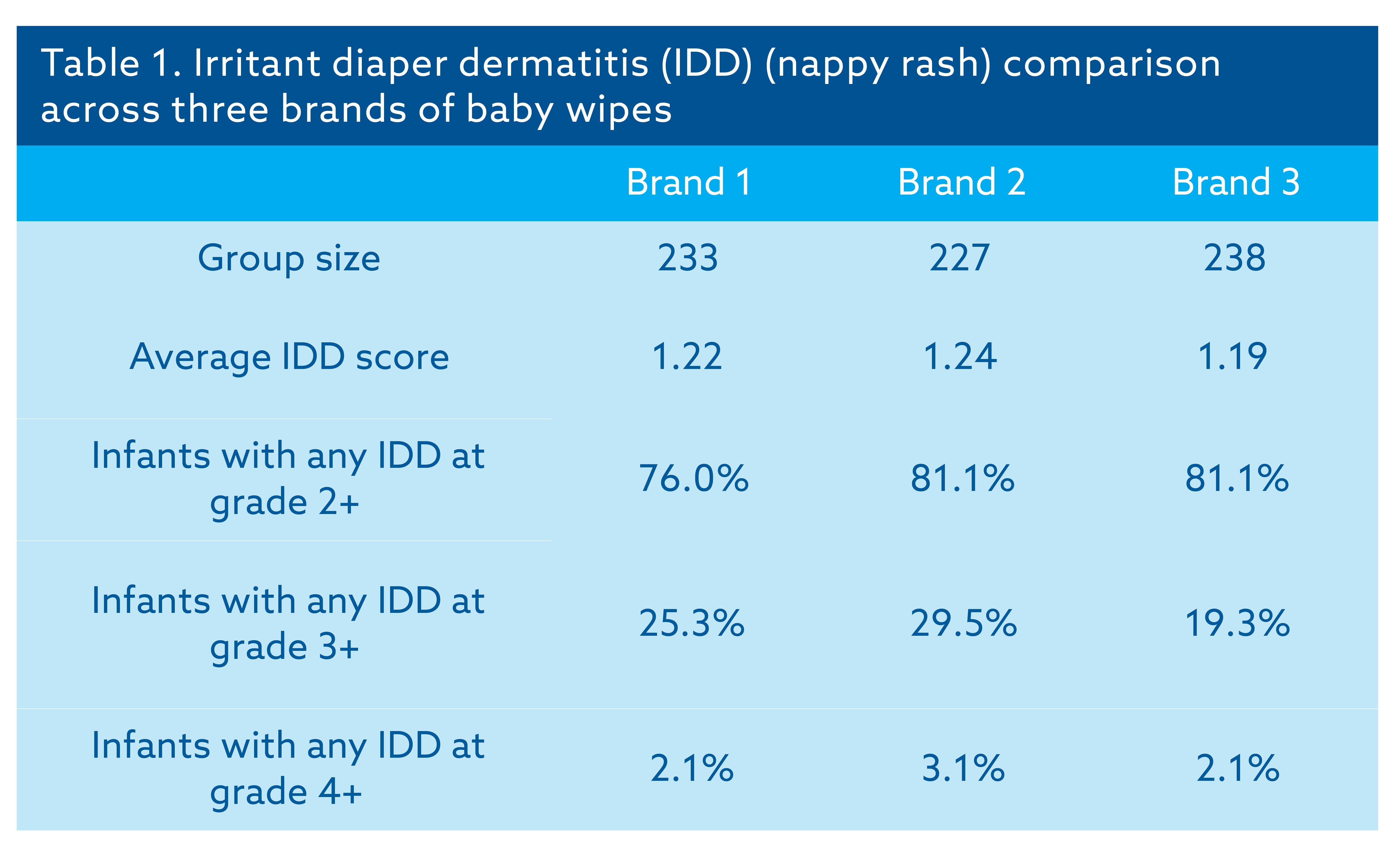
different formulations. When incidence of rash was analysed across all
three brands, findings indicated that babies cleansed with Brand 3
demonstrated the lowest incidence of IDD (19%) followed by Brand 1
(25%) and Brand 2 (30%). IDD also cleared more quickly in babies
assigned to the Brand 3 study arm. For each one day of IDD in babies in
the Brand 3 group, nappy rash lasted 1.48 days with Brand 1 and 1.69
days with Brand 2. The finding that babies who were cleansed with the
brand of wipes containing the fewest ingredients had fewer days of IDD
than babies who were cleansed with the other two brands of wipes is
clinically significant; this represents the first research evidence of brand
as a determinant of skin integrity during the first eight weeks of life as
reported in an initial publication (Price et al, 2020).
Discussion
We are confident that the accuracy of assessment was high in this study
due to the daily surveys and the involvement of mothers as co-
researchers in holding complete responsibility for observation, assessment and recording data. Some previous studies used professional assessment of skin integrity or hydration (Visscher et al, 2009) or a
combination of professional and parental assessment (Lavender et al, 2012) while other studies relying solely on parental assessment
(Goldman and Lodhi, 2016) have used retrospective data collection which has been shown to be less accurate than contemporaneous feedback in other areas of research (Monk et al, 2015).
Clinically significant IDD was identified as level 3 on the assessment scale. A severe rash scoring 4 or 5 was rare, with only 2.4% of babies experiencing this. The overall average nappy rash score on the IDD scale was 1.43, with babies experiencing on average 21 days of rash out of a
total of 55 days. Gender, parity and maternal age were all significant factors, with male babies experiencing a higher number of days with IDD, as did babies who were born to multiparous mothers, and babies whose families reported higher than average family income (≥ £30 000 pa).This
contradicts a previous study from the US that identified lower than average income as a risk factor for IDD (Smith et al, 2013).The impact on
low-income families of the cost of nappies may have been a factor in a reduced number of nappy changes carried out over 24 hours in the US
research.
Reducing nappy use by less frequent changing was not a factor in the present study, as all products were supplied free of charge. The relationship between income and IDD requires further investigation as a hypothesis could be made that it relates to feeding method. Higher
income mothers tend to have higher breastfeeding rates (National Institute for Health and Care Excellence, 2014), although socioeconomic
disadvantage does not appear to reduce breastfeeding in black and minority ethnic communities (Oakley et al, 2013). While breastfeeding can be a protective factor against IDD over the entire nappy wearing period (Yoshioka et al, 1983; Stamatas and Tierney, 2014) in the early weeks of life, breastfed babies pass stools more frequently and presence of fecal material is a risk factor for IDD (Visscher, 2009).
Although feeding data were not collected in the daily survey, in order not to make women feel uncomfortable about their choice of method, information about intended feeding method was recorded on recruitment to the study. The final survey collected data on feeding method in the last week of the study. Therefore, although there is no
way of determining when mothers who intended to breastfeed but ended the study using formula changed feeding methods, it can be assumed that mothers who expressed intent to breastfeed and were still breastfeeding in the final week of the study remained consistent in their
feeding method throughout the eight-week period. This was confirmed in data collected through qualitative interviews with approximately 5% of the total sample. Mothers who indicated a strong intention to breastfeed were more likely to end the study still breastfeeding, where mothers who expressed doubts about breastfeeding, intention to use mixed methods, or intention to formula feed spent a very brief amount of time, if any,
attempting to breastfeed.This information may be of use to midwives when providing prenatal information on infant-feeding methods, as early
frequent soft stools are normal and should not influence mothers regarding feeding methods.
Instead, breastfeeding mothers can be reassured about the benefits of
breastfeeding and encouraged to change the baby’s nappy every time they pass fecal material, even if this is only a small amount. Breastfeeding
mothers, and indeed all mothers, could also be encouraged to allow the
baby more nappy free time as air circulation is known to lower the skin pH which helps to reduce the incidence of IDD (Visscher, 2009; Li et al, 2012).
Ethnicity may also be a factor as infants of mothers who self-identified as ‘mixed race’ according to the UK census classifications had lower rates of IDD than infants of ‘white’ mothers.
This was not true of mothers identifying as ‘black’ or ‘Asian’ warranting further investigation into biological factors, such as skin pigmentation,
versus cultural factors, such as traditional skincare or bathing routines. The ethnic origin of women in the study was similar to distribution in
the area census data, although the total percentage of women from minority ethnic backgrounds was higher than that of people in the
wider population. This may be because the study sample consisted only of pregnant women where area census data included people of all ages and genders (Office for National Statistics, 2016).
Appendix 2. Final (day 56) survey
1. Which brand of wipe were you given to use during the duration of the study?
Brand 1, Brand 2, Brand 3, more than one brand of wipe
2. How did you give birth?
Normal vaginal birth, forceps/ventouse, breech birth, caesarean section
3. What was your baby’s birth weight?
Less than 5lb 5oz, 5lb 5oz−6lb 6oz, 6lb 7oz−7lb 16oz, 8lb 0oz−9lb 2oz, 9lb 3oz−10lb 6oz, equal to or greater than 10lb 7oz
4. In the last week of your participation in the study, which method of feeding did you use to feed your baby?
Breast, formula, mixed
5. In the last week of your participation in the study, can you estimate how many wipes you used at each nappy
change when your baby had urinated (‘wee’) only?
Half a wipe, 1 wipe, 2 wipes, 3 wipes, 4 wipes, 5 wipes, 6 wipes, 7 or more wipes
6. In the last week of your participation in the study, can you estimate how many wipes you used at each nappy
change when your baby had done a stool (‘poo’)?
Half a wipe, 1 wipe, 2 wipes, 3 wipes, 4 wipes, 5 wipes, 6 wipes, 7 or more wipes
Section B. Further questions about your baby
Please answer this section thinking about since your baby was born
7. Has your baby had any signs of nappy rash since birth?
Yes/No
8. Have you used any creams in the nappy area of your baby since your baby was born?
Yes/No
9. What did you use this nappy cream/s for?
Routinely to prevent nappy rash, only to heal an existing rash, only when prescribed for thrush, other
10. Has your baby taken any antibiotics since birth?
Yes/No
11. Aside from your midwife/health visitor, since birth, have you taken your baby for an appointment with a doctor
or nurse to raise concerns about your baby’s skin in the nappy area?
Yes/No
12. Have you used any other brand of wipes aside from the one given to you during the duration of the study (the eight weeks)?
Yes/No
13. How often do you give your baby a bath/body wash (on average)?
More than once per day, once per day, every 2 days, every 3 days, once a week, less than once a week
14. How often do you change your baby’s nappy during the day?
Hourly, every 2 hours, every 3 hours, every 4 hours, 5 hours or more
15. In the past four weeks, who did the majority of nappy changes for your baby?
Baby’s mother, baby’s father, baby’s grandparent, baby’s nanny (paid carer), other person
16. Which type of washing powder/liquid did you use to wash your baby’s clothes?
Biological, non-biological, biological and non-biological, don’t know type of washing powder/liquid, I did not use a
washing powder/liquid
Section D: Question about the wipes given to you to use
17. How did you find the scent/smell of the wipes?
Extremely unpleasant, moderately unpleasant, slightly unpleasant, neither unpleasant, nor pleasant, slightly pleasant,
moderately pleasant, extremely pleasant
18. Do you believe these baby wipes helped prevent nappy rash for your baby?
Yes/No/made no difference/unsure
19. How well do you believe these wipes cleaned your baby’s skin?
Better than expected, as well as expected, less well than expected
20. Do you think using this brand of wipes is more convenient than using cotton wool and water to clean your baby?
Yes/No/makes no difference in terms of convenience
21. In relation to the wipes you were given to use in this study, would you say:
Overall I liked using this wipe, overall I did not mind using this wipe, overall I disliked using this wipe
22. Would you recommend this brand of baby wipes to a friend?
Definitely wouldn’t, probably wouldn’t, probably would, definitely would
23. In the next two months, for the majority of nappy changes, do you plan to:
Continue using this brand of wipes, use a different brand of wipes, use cotton wool and water, use something else
24. If you said you plan to use a different brand of wipes, what are the reasons for this?
Too expensive, caused skin irritation, poor experience of using the wipes, hard to find this brand in shops, I prefer
another brand, other
Effect on the environment
Cost of the product
Recommendation from healthcare professional
Recommendation from family/friends
Recommendation on an advert or online
Convenience/ease of use
How it makes my baby smell
How well it cleans my baby
Natural ingredients in the wipes
Other
The primary outcome for which the study was designed was to determine whether there were any differences in rates of IDD between brands of baby wipes used (Table 1). As this study was designed as ‘real-world research’ (Robson and McCartan, 2016), no restrictions were placed on mothers regarding infant skincare practices.
Although the study was midwifery led, it was made clear to participants that the principle investigator and co-investigator were not available to provide midwifery advice to participants; mothers were advised to seek information from their own midwives. Mothers were not instructed by the
study team on how often to change nappies, when or how often to bathe their babies, or what products to use, including infant-bathing products
or skin creams, to treat or prevent nappy rash.
When these factors and others, such as the use of biological or non-biological washing powders, were compared, there were no differences across the three arms of the study. Therefore, differences in incidence of rash were highly likely to be attributable to the baby wipe product used.
Key points
● Mothers acted as co-researchers, collecting and reporting daily
survey data
● Greatest intensity of data collection for this size of sample
● Previous studies cited into skin integrity and hydration were also
industry funded
● Characteristics of study arms consistent, indicating wipe formulation as
significant predictor of rate of irritant diaper dermatitis
Conclusion
Although previous studies have answered the question as to whether the use of baby wipes is as safe from birth as water with cotton wool or
cloth, no previous study has answered the question as to whether there is any clinically significant difference between brands, thus identifying this as a question of scientific interest.
The BaSICS study has achieved this with a large cohort of mothers and babies, aged from birth to eight weeks old, and a comprehensive volume of survey responses. It has been noted that the quality of a survey can be judged not only by good design but also by reporting findings in a
way that does more than just reiterate the data (Kelley et al, 2003).
The BaSICS team asserts that this has been achieved and that the findings of this study will be of interest to midwives, dermatologists, paediatric nurses, parents and manufacturers of baby products. BJM
Declaration of interests: The authors declare that they have no conflict of interest.
CPD reflective questions
Irritant diaper dermatitis (IDD) or nappy rash tends to increase during the
weaning/teething stages of a baby’s life.
- What are some reasons researchers might want to investigate nappy rash in the first eight weeks of life?
- What was the overall rate of IDD in this study and how does that compare to other reported rates of nappy rash?
- What are the advantages/disadvantages of asking mothers to collect
skincare data rather than by researcher assessment?
- Is there a relationship between socioeconomic status or ethnicity and
incidence of IDD? Why might this be important information for midwives?
- What is ‘real-world research’ and how does this differ from a clinical trial?
- What are the advantages/disadvantages for its use in this study?
References:
Ehretsmann C, Schaefer P and Adam R. Cutaneous tolerance of baby wipes by infants with atopic dermatitis and comparison of the mildness of baby wipe and water in infant skin. Journal of the European Academy of Dermatology and Venereology (JEADV). 2001;15(1):16–21. https://doi.org/10.1046/j.0926-9959.2001.00004.x
Furber C, Bedwell C, Campbell M, Cork M, Jones C, Rowland L and Lavender T. The challenges and realities of diaper area cleansing n for parents. JOGNN. 2012; 41:E13–E25. https://doi.org/10.1111/j.1552-
6909.2012.01390.x
Garcia Bartels N, Lünnemann L, Stroux A, Kottner J, Serrano J, Blume-Peytavi U. Effect of diaper cream and wet wipes on skin barrier properties in infants: a prospective randomized controlled trial. Pediatric Dermatology. 2014; 31(6):683–691. https://doi.org/10.1111/pde.12370
Goldman M, Lodhi I. A real-world evidence study evaluating treatment for nappy rash. British Journal of Nursing. 2016; 25(8). https://doi.org/10.12968/bjon.2016.25.8.432
Jones SR, Carley S, Harrison M. An introduction to power and sample size estimation. Emergency Medicine Journal. 2003; 20:453–458.
https://doi.org/10.1136/emj.20.5.453
Kelley K, Clark B, Brown V, Stizia J. Good practice in the conduct and reporting of survey research International Journal for Quality in Health Care. 2003; 15(3):261–266. https://doi.org/10.1093/intqhc/mzg031
Lavender T, Furbur C, Campbell M,Victor S, Roberts I, Bedwell C, Cork MJ. Effect on skin hydration of using baby wipes to clean the napkin area of newborn babies: assessor blinded randomized controlled equivalence trial. BMC Pediatrics. 2012; 12:59. https://doi. org/10.1186/1471-2431-12-59
Lewis-Beck, MS, Bryman A, Futing Liao, T. The SAGE encyclopedia of social science research methods. Thousand Oaks, CA: Sage Publications, 2004. https://dx.doi. org/10.4135/9781412950589
Li CH, Zhu ZH, Dai YH. Diaper dermatitis: a survey of risk factors for children aged 1-24 months in China. The Journal of International Medical Research. 2012; 40:1752–1760. https://doi.org/10.1177/030006051204000514
Monk RL, Heim D, Qureshi A, Price A. ‘I have no clue what I drunk last night’: using smartphone technology to compare in-vivo and retrospective reports of alcohol consumption PlOS ONE. 2015; 10. https://doi.org/10.1371/journal.pone.0126209
National Institute for Health and Care Excellence. Maternal and child nutrition. 2014. https://www.nice.org.uk/ guidance/ph11/chapter/2-
public-health-need-and-practice (accessed 10 June
2020)
Oakley LL, Renfrew MJ, Kurinczuk JJ, Quigley MA. Factors associated with breastfeeding in England: an analysis by primary care trust. BMJ Open. 2013; 3(6). https://doi. org/10.1136/bmjopen-2013-002765
Office for National Statistics. Census aggregate data. UK
Data Service, 2016 Philipp R, Hughes A, Golding J. Getting to the bottom of nappy rash. British Journal of General Practice. 1997; 47:493–497

Expert care for every delicate skin story
From daily diapering tips to deep dives into skin science, explore our Advice & Care guides and our dedicated Skin Care Hub!💧✨