Select your region
-
Europe
-
Americas
-
Africa and Middle East
-
Asia Pacific
Cleaning the newborn diaper area: a literature review
New parents often face a dilemma: healthcare professionals generally recommend using cooled boiled water and cotton balls, while baby wipes, with their varying compositions, are often the subject of conflicting advice. This literature review will examine our current understanding of newborn skin, diaper rash, and evidence-based diaper area cleansing practices.

Introduction
The skin in the diaper area of a newborn is a unique environment, exposed to a combination of irritants such as urine, feces, obstruction, and frequent washing. As a result, infant contact dermatitis affects up to 25% of diaper-wearing infants during the first four weeks of life. 1
New parents often face a dilemma: healthcare professionals generally recommend using cooled boiled water and cotton balls, while baby wipes, with their varying compositions, are often the subject of conflicting advice. This literature review will examine our current understanding of newborn skin, diaper rash, and evidence-based diaper area cleansing practices.
neonatal skin structure
The structure and function of a newborn's skin change rapidly during the first few weeks of development. The baby's skin is subject to greater insensible water loss (IWL) and reduced hydration of the stratum corneum, resulting in a less effective skin barrier. 2
Skin pH decreases during the first 1 to 4 days of life and continues to decrease during the first three months. A higher skin pH in infants can reduce the integrity of the stratum corneum and increase sensitivity to mechanical trauma. Skin pH in the diaper area has been shown to be higher than in other areas in newborns compared to day 14. 3
The unique environment of the diaper area and its implications for newborn skincare
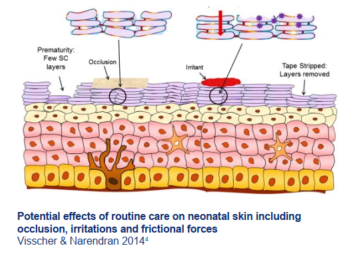
Routine skincare can cause friction and irritation from cleansers and wipes. 2 In addition, the diapers themselves keep the skin in a moist and occlusive state. 4
Effective newborn skincare for diapers
Skin care for infants who are fed in diapers requires adequate cleansing of physiological irritants while preserving the skin barrier function and avoiding physical damage, irritation, or potential allergic contact dermatitis in reaction to exogenous chemicals. 5
Diaper area cleaning practices – Cotton and water or wipes?
In the UK, the use of cotton and water is generally recommended to parents by midwives and childcare nurses.⁶ However, to date, five studies have demonstrated comparable, or even superior, effectiveness of baby wipes compared to water and cotton balls for cleaning a baby's skin after diaper changes.⁷⁻¹²
Parents are ready to adopt baby wipes 13
Water alone may not be sufficient for adequate purification.
- Easier to pack
- Practical
- Maintaining consistent water quality even far from home
What is the impact of the formulation of wipes?
A recent prospective study (the BaSICS study) compared the effects of three different brands of baby wipes on the incidence and duration of moderate to severe diaper rash (diaper dermatitis) from birth to eight weeks. 12 The study showed that babies cleaned with the brand containing the fewest ingredients (ultrapure water and fruit extract only) had fewer days of clinically significant diaper rash. This suggests that using wipes with the minimal composition offers an additional benefit. 14
Duration of moderate to severe diaper rash in the BaSICS study compared to that of brand 3 (brand containing the fewest ingredients) 14

The importance of water quality
In the UK, 60% of the population lives in areas with hard water. 15 Studies suggest that softened or ultrapure water helps maintain skin barrier function, compared to tap water, particularly in newborns predisposed to atopic dermatitis. 16–18 Proposed mechanisms to explain this phenomenon include increased detergent deposition on the skin, altered calcium signaling, and increased skin pH—all factors that can impair skin barrier function. 18
Properties of purified water16
- No bacteria/microorganisms
- No trace of minerals such as magnesium and calcium, which contribute to water hardness.
- pH lower than that of tap water (5 versus 7)
Conclusions
- Using wipes to clean the diaper/changing area appears comparable to, or even superior to, methods using water and cotton/rags.
- A recent study supports the use of wipes with minimal ingredients (ultra-pure water and fruit extract only) in the prevention of diaper rash.
References
- Philipp R, et al. Br J Gen Pract 1997;47:493–497;
- Chiou YB, Blume-Peytavi U. Skin Pharmacol Physiol 2004;17(2):57-66;
- Visscher MO, et al. Clin Dermatol 2015;33(3):271-280;
- Visscher M, Narendran V. Newborn Inf Nurs Rev 2014; 14(4):135-41;
- Collier M. British Journal of Nursing 2016;25(20):26-32;
- National Institute for Excellence in Health and Care. Postnatal care up to 8 weeks after birth [CG37] [online] 2006. Last accessed 01.09.21 - Available from: https://www.nice.org.uk/guidance/cg37;
- Rodriguez KJ, et al. Pediatric Dermatology. 2020; 37: 447-454;
- Ehretsmann C, et al. J Eur Acad Dermatology Venereol 2001;15(Supplement 1):16-21;
- Lavande T, et al. BMC Pediatrics 2012;12(59);
- Adam R, et al. Pediatr Dermatol 2009;26(5):506-13;
- Visscher M, et al. Neonatology 2009;96(4):226-234;
- Garcia Bartels N, et al. Pediatric Dermatol 2012; 29: 270-276;
- Furber C, et al. J Obstet Gynecol Neonatal Nurses 2012;41(6):E13-25;
- Price A, et al Pediatr Neonatol 2021;62(2):138-145;
- Source: Thames Water UK;
- Jabbar-Lopez ZK et al. BMJ Open 2019;9(8):e027168;
- Tanaka A, et al. Acta Derm Venereol 2015;95:787-791;
- Danby SG, et al. J Invest Dermatol 2018;138(1):68-77.

Expert care for every delicate skin story
From daily diapering tips to deep dives into skin science, explore our Advice & Care guides and our dedicated Skin Care Hub!💧✨