Select your region
-
Europe
-
Americas
-
Africa and Middle East
-
Asia Pacific
The BaSICS (Baby Skin Integrity Comparison Survey) study:
A prospective experimental study using maternal observations to inform on the effect of baby wipes on the incidence of irritant diaper dermatitis in infants, from birth to eight weeks of age.
Get overview of this article
The BaSICS (Baby Skin Integrity Comparison Survey) study investigated the impact of different brands of baby wipes on the incidence of irritant diaper dermatitis (IDD) in infants from birth to eight weeks. Conducted with 722 eligible participants, the study compared three brands of wipes, each marketed for newborns but differing in ingredient composition. Mothers reported daily on their baby's skin condition using a smartphone app. Results showed that 24.6% of infants experienced diaper rash, with those using the brand with fewer ingredients reporting significantly fewer days of clinically significant rash (score 3 or more). Severe IDD was rare (2.4%). The findings suggest that gentle formula baby wipes are safe for infants and highlight the effectiveness of using mobile apps for real-time data collection on skin conditions.

Background : Baby wipes have been shown to be safe and effective in maintaining skin integrity compared to water alone. However, no previous study has compared different wipe formulations. The aim of the BaSICS study was to identify potential differences in the incidence of irritant diaper dermatitis (IDD) in infants using three different brands of wipes, all marketed as suitable for newborns, but containing varying amounts of ingredients.
Methods: Women were recruited during the prenatal period. Participants were randomly assigned to receive one of three brands of baby wipes for use during the first eight weeks postpartum. All participants received the same diapers. Participants reported daily on their baby's skin integrity on a scale of 1 to 5 using a customized smartphone app. Analysis of the brand effect on the incidence of clinically significant diaper rash (score of 3 or more) was performed using a generalized negative binomial linear model, controlling for potential confounders at baseline. Analysts were blinded to the wipe brand. Results: Of 737 women enrolled, 15 were excluded (admitted to neonatal intensive care, preterm, or other infant health problems). Of the 722 eligible infants, 698 (97%) remained in the study for the full 8 weeks, 24.6% of whom experienced diaper rash at some point during the study. Mothers who used the brand with fewer ingredients reported fewer days of clinically significant diaper rash (score 3) than participants who used the other two brands (p < 0.002 and p < 0.001). Severe IDD (grades 4 and 5) was infrequent (2.4%).
Conclusions: The low incidence of severe diaper rash suggests that gentle formula baby wipes are safe for cleaning infants from birth to eight weeks of age during diaper changes. The brand with fewer ingredients resulted in significantly fewer days of clinically significant diaper rash. Daily observations recorded on a smartphone app proved to be a highly acceptable method for obtaining real-time data on diaper rash.
Clinical trial registration: This study was not designed or registered as a clinical trial, as no intervention was made in usual infant care practices. Mothers who had already chosen to use disposable diapers and wipes agreed to observe and report on their infants' skin condition; in return, they received a free nine-week supply of diapers and wipes. Copyright © 2020, Taiwan Pediatric Association. Published by Elsevier Taiwan LLC. This is an open access article licensed under CC BY-NC-ND 4.0 (http://creativecommons.org/licenses/by-nc-nd/ 4.0/).
1. Background
Irritant diaper dermatitis (IDD, also known as diaper rash) is a skin condition characterized by inflammation of the buttocks, groin, and perineum. It is caused by contact with urine and feces, combined with friction from the diaper against the skin¹ and is one of the most common skin conditions in infancy, although international prevalence estimates show wide variation in IDD rates.²⁻⁹ Healthcare professionals have traditionally recommended water with cloth or cotton wipes to cleanse the diaper area of infants; However, two pivotal studies have not shown increased skin irritation when using baby wipes.10,11 In addition, baby wipes were associated with decreased skin irritation compared with cloth wipes10 and parents reported that baby wipes were more convenient to use than cotton balls and water.11 Both studies recommended further research on the impact of baby wipes on infant skin, especially studies comparing different baby wipe formulations.10,11
Baby wipe formulas have improved significantly over the past 40 years: harsh ingredients such as isopropanol are no longer added, and many brands exclude perfume, as recommended by the National Institute for Health and Care Excellence (NICE).12e14 The brands used in this study were marketed as gentle enough for newborn skin, but differed in the number of ingredients. Brand three contained two ingredients,15 while brands one and two each had more than three times as many.
2. Methods
2.1. Design
The BaSICS (Baby Skin Integrity Comparison Survey) was a prospective experimental study designed to compare three different brands of baby wipes, using maternal observations of the incidence of developmental skin disorders (DSD) in infants from birth to eight weeks of age. Greater Manchester was selected as the study site due to its multi-ethnic demographic profile. Pregnant women expecting a single, healthy, full-term baby were recruited during the prenatal period through direct contact or advertisements in hospital prenatal clinics and on social media.
2.2. Sample size calculation
Sample size calculations indicated that, to detect a difference between a 15% prevalence of IDD in one brand of baby wipes and 5% in another brand, 166 participants per group were required (a total of 498, assuming 80% power and a 5% type I error rate). Assuming a 70% retention rate, the study aimed to recruit 700 women.
2.3. Randomization
The mothers and babies were randomly assigned to one of three brands of baby wipes; all mothers received the same brand of disposable diapers. The researchers involved in the data analysis were unaware of the wipe brand. Blinding the participants was not possible, as this would have required repackaging the wipes, which could have affected the quality of the contents.
2.4. Procedure
A starter pack containing a weekly supply of diapers and wipes was provided to all participants upon registration for the study, starting at week 34 of gestation. This ensured that mothers had an adequate supply of their allotted wipes to use immediately after their baby's birth. Subsequently, diapers and wipes were delivered to participants' homes by courier as soon as they voluntarily enrolled in the study by completing their initial survey, and then at approximately two-week intervals throughout the study period. Each mother received a free nine-week supply of diapers and wipes and, in return, completed a short daily survey from the day of her baby's birth until the child was eight weeks old (Appendix). The mothers' daily observations were recorded using a mobile application specifically designed for this purpose; a paper version of the survey was made available for the small number of participants who preferred this method (n = 3).
2.5. Statistical analysis
The main outcome of interest was the incidence of significant IDD in the sample and the comparisons of incidence among the three groups. IDD was measured on a scale of 1 to 5, where grade 1 indicates no redness or rash,
Comparative survey on the integrity of baby skin 139
Grade 2: mild redness and rash; grade 3: the point at which cracked skin and discomfort are evident; and grades 4 and 5: more severe (Appendix). The outcome of "clinically significant intimate hygiene disease" was defined as grade 3 or higher. Data were analyzed using SPSS and Stata. Univariate comparisons between wipe brands and sample characteristics were performed using ANOVA, chi-square, and Kruskal-Wallis tests, depending on the variable type. Analyses of the effect of brand on the incidence of intimate hygiene disease used a generalized negative binomial linear model with a logarithmic link function, controlling for potential confounders at baseline. 16
3. Results
3.1. Sample characteristics
Recruitment continued until 737 women enrolled in the study. Fifteen infants were ineligible at birth (eight required a stay in neonatal intensive care, one was born prematurely, two had other infant health problems, and four were excluded for multiple criteria), leaving 722 women and their infants eligible to begin the study. Retention was much higher than expected, with only 24 participants dropping out, leaving an analysis population of 698 women who completed the study (96.7%), confirming the validity and acceptability of the study methods. Dropout was similar across the three groups, with 11 participants dropping out from group one, 8 from group two, and 5 from group three (χ² Z 2.25, p Z 0.32).
Brand 1 was used by 233 participants, brand 2 by 227, and brand 3 by 238. The number of participants in each group varied because: i) participants were assigned a brand during the prenatal period, but some babies subsequently did not qualify; ii) dropout rates were slightly different between groups; and iii) the original randomization did not start with an exactly equal number because of the block randomization process.
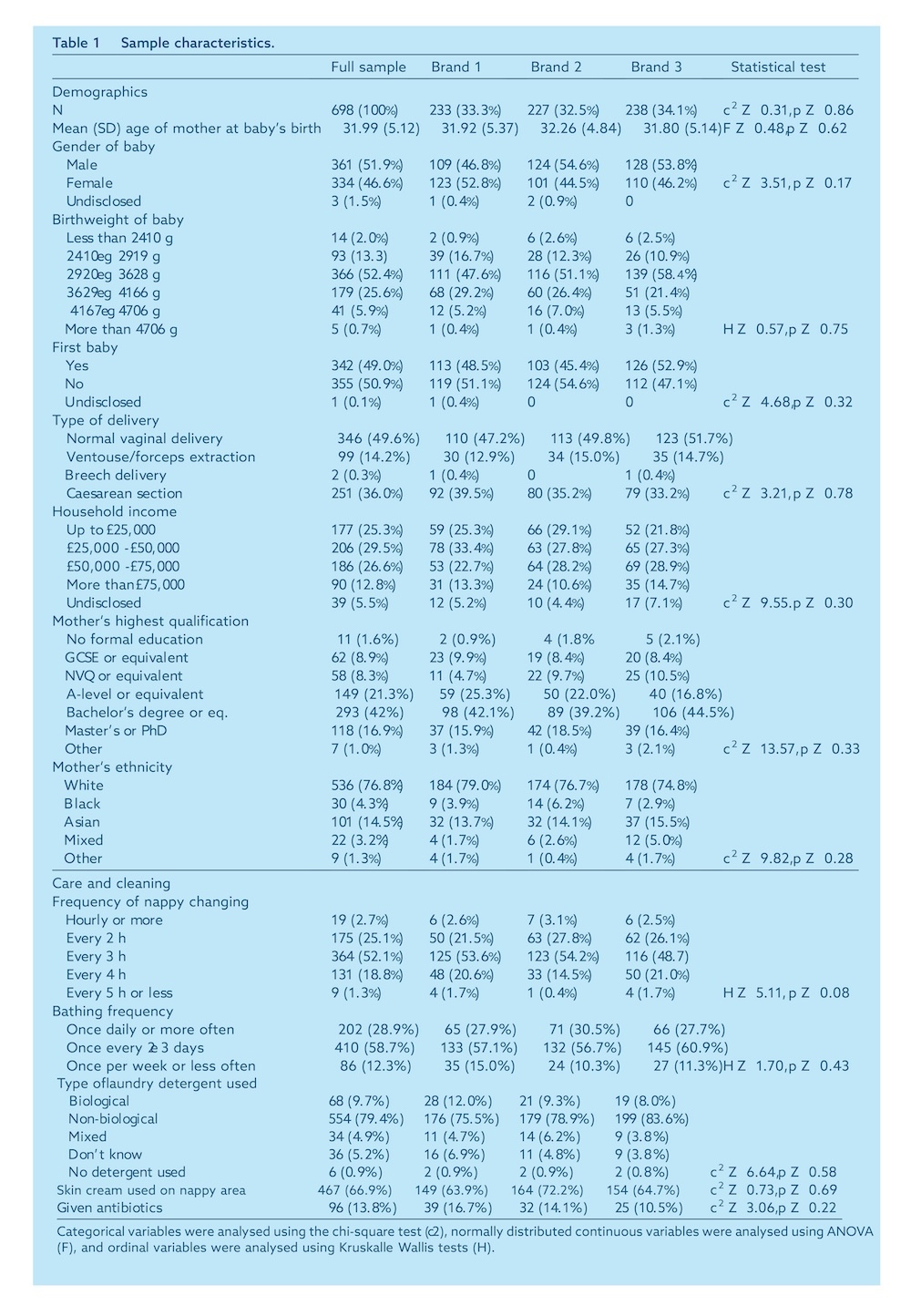
Table 1 shows the demographic characteristics and details of childcare and hygiene routines for the population analyzed and for each group. The average age of the mothers at the birth of their babies was 32.0 years (SD Z 5.12), and slightly more than half (51.9%) of the babies were male. Slightly less than half (49.0%) of the babies were their mothers' first child, and slightly less than half (49.6%) were born via normal vaginal delivery. Ethnicity was determined using UK government census classifications; 75% of the mothers in this sample self-identified as White, 15% as Asian, 5% as Black, 3% as mixed race, and 1% as another ethnic group. Comparison with population data for Greater Manchester17 showed that there was a higher proportion of people from ethnic minorities in the sample (23.3%), compared to the general population (16.4%; χ²Z25,36,p<0.001). This may be due to differences in age ranges: census data include people of all ages, whereas our sample consisted only of women of childbearing age.
More than half of the participants (52.1%) changed their babies' diapers approximately every 3 hours, and the majority (58.7%) bathed them once every 2 or 3 days. Many (79.4%) used non-biological laundry detergent, and two-thirds of the participants (66.9%) reported using diaper rash cream on their babies at some point during the study. A minority (13.8%) of the babies received antibiotics at some point during the study. No differences were observed between the groups in any of the characteristics shown in Table 1.
3.2. Analysis of the main results
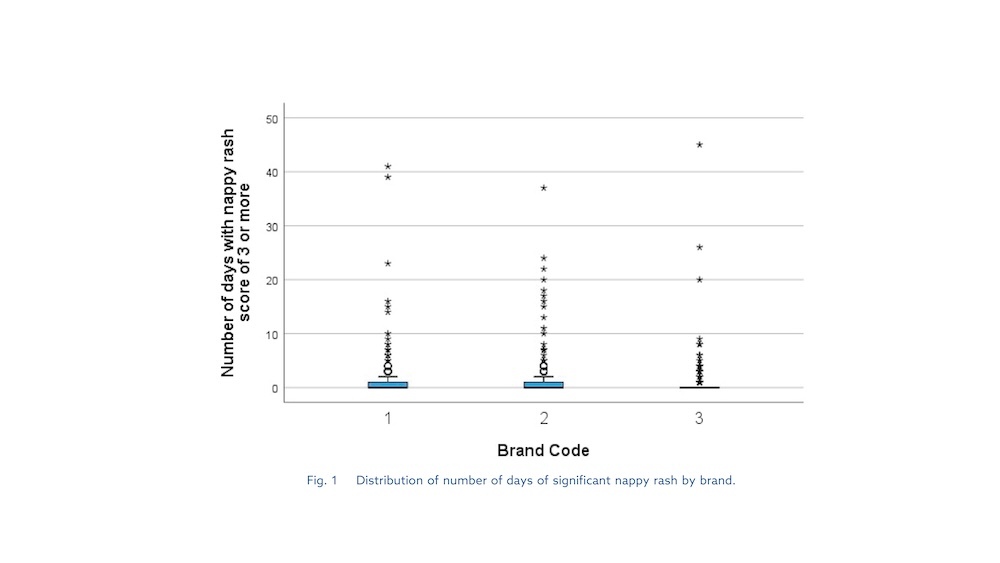
The percentage of mothers who reported at least one day of clinically significant diaper rash (grade 3 or higher) was 24.6%. Brand 3 had the lowest proportion of infants with significant diaper rash (n = 46; 19%), followed by Brand 1 (n = 59; 25%) and Brand 2 (n = 67; 30%). The distribution of the number of days with significant diaper rash by brand is shown in Figure 1. Severe diaper rash (grades 4 and 5) was infrequent (2.4% of infants). There were no reports of any problems such as allergic reactions requiring medical attention. Overall, the mean diaper rash score was 1.43, and the mean number of days without diaper rash was 34 out of the 55 days in the study.
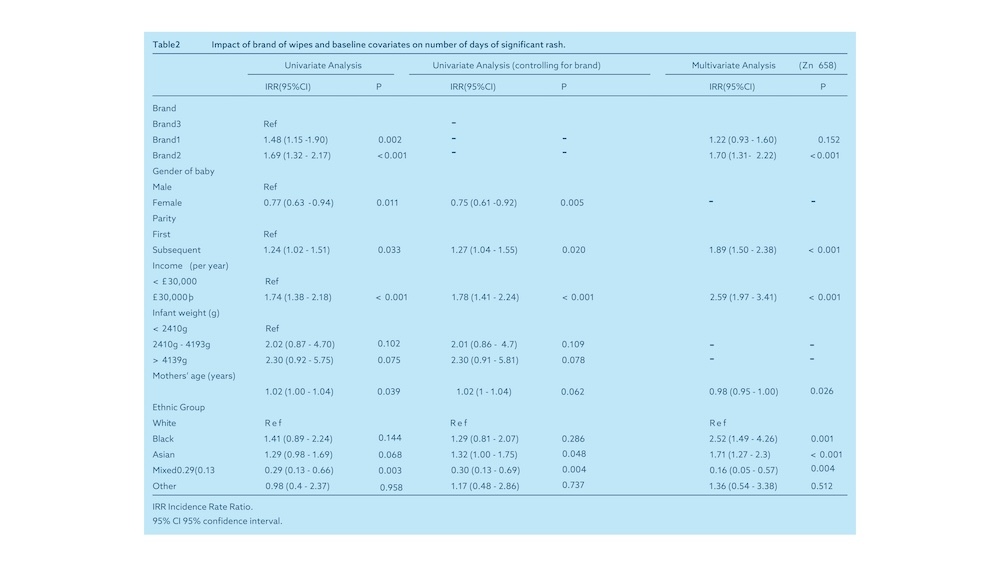
A univariate analysis (Table 2) of clinically significant IDD showed a highly significant brand effect. For one day of clinically significant diaper rash with Brand 3, the rash would have lasted 1.48 days (95% CI: 1.15–1.90) with Brand 1 (p Z 0.002) and 1.69 days (95% CI: 1.32–2.17) with Brand 2 (p < 0.001). Other potential factors included infant sex (girls had a lower rash rate, incidence rate ratio [IRR] 0.77, 95% CI: 0.63–0.94, p Z 0.011) and parity (second or subsequent infants had a higher rate: IRR 1.24, 95% CI: 1.04–1.51, p Z 0.033). Each additional year of maternal age was associated with a 1.02-fold increase (95% CI: 1.00–1.04) in the rate of significant diaper rash (p < 0.039). Those with above-average annual household income (>£30,000) had a higher rate of diaper rash than those reporting below-average household income (IRR 1.74, 95% CI: 1.38–2.18, p < 0.001). Infants whose mothers were of mixed ethnicity had a lower rate of diaper rash (IRR 0.29, 95% CI: 0.13–0.66, p < 0.003) compared with infants of white mothers.
A second set of models tested each covariate separately, controlling for brand. Infant sex, parity, and household income remained significant. A multivariate forward stepwise regression model yielded similar results for the main analysis. Wipe brand remained a significant predictor of the number of days of rash, with Brand 2 use having a significantly higher rash rate (IRR 1.70, 95% CI 1.31–2.22, p < 0.001) compared with Brand 3. Although Brand 1 also had a higher rash rate compared with Brand 3, this was no longer statistically significant (IRR 1.22, 95% CI 0.93–1.60, p < 0.152). Compared with first babies, later babies had a higher rate of rash (IRR 1.89, 95% CI: 1.50-2.38, p < 0.001) and those with above-average family income also had a higher rate of IDD (IRR 2.59, 95% CI: 1.97-3.41).
3.3. Fidelity to treatment
Loyalty was measured by the number of days of exclusive use of the assigned brand of wipes for diaper area cleaning. Overall, 59.5% of participants reported 100% loyalty to their assigned brand of wipes. An additional 28.3% used a different cleaning method for 1 to 5 days; 12.2% reported using a different cleaning method for more than 5 days, and 2% reported using a different method for more than 10 days. Other methods used included cotton and water (used at least once by 25.5% of participants), another brand of wipes (12.9%), water only (11.5%), or any other method (6.6%). There was no difference in loyalty between the groups (χ²Z = 3.03, p = 0.22).
4. Debate
4.1. Main result
This study was designed to compare three brands of baby wipes for their impact on intellectual disability. One of the brands, Brand 3, contained fewer ingredients than the other two. The results showed that babies wiped with Brand 3 were less likely to have clinically significant intellectual disability than those wiped with the other two brands.
4.2. Strengths and limitations
Since it was not possible to conceal the brands received from participants, the possibility that participants' observations of diaper rash (DPR) were biased by perceptions or prior experiences with wipe brands is acknowledged. Measurement error, as a source of bias, was reduced by using real-time (rather than retrospective) reporting of DPR. The vast majority of those eligible for the study (97%) were retained and analyzed, and all participants contributed 55 days of continuous daily observations of their infants' skin condition. This high retention and protocol compliance rate was attributed to two factors: incentives in the form of free diapers and wipes, and the ease of use of the smartphone app, which reminded parents to submit daily observations and was simple and quick to use. The use of daily reports from mothers was innovative, providing some important benefits. Previous studies in the UK on diaper rash have relied on a single retrospective survey of parents,4,5 or on a single or repeated assessment by a medical professional.11 Although there have been studies with significantly larger sample sizes,6 no other study has carried out this level of data collection for a large sample of infants. Mothers were able to report on diaper rash daily, in real time, via a user-friendly interface on their smartphone, which contained reference charts for assessing IDD on a five-point scale. This allowed mothers to reflect daily on their baby's skin condition and cleaning routines using real-time data collection methods, which are known to be more accurate than retrospective methods.18 This has resulted in an IDD dataset that, to the authors' knowledge, is the most comprehensive to date for younger infants. The lack of direct professional involvement, including visits to clinics, may have helped retain participants, contributing to the high study completion rate.
4.3. Prevalence of intellectual and developmental disability
The prevalence of IDD in the first eight weeks of an infant's life observed in this study (24.6%) is close to that of a previous UK study,5 which found a prevalence of 25% (based on a sample of 12,103 infants) and higher than that of another UK study,4 whose prevalence rate was 16% (based on a sample of 532 infants). These differences may be methodological, as IDD measurement techniques have not been consistent. None of these previous studies collected daily data, but rather used retrospective questionnaires at four weeks5 or up to two years of age.4 Therefore, it is difficult to conclude whether the prevalence was high, low, or typical in this sample. It is also important to note the distinction between the different degrees of IDD severity. In this study, the primary outcome was based on clinically significant IDD, which was defined as grade 3 or higher on a 5-point scale. Severe IDD (grades 4 and 5) was rare (2.4% of participants reported any severe rash). Future studies should consider the severity of IDD.
5. Conclusion
This large-scale study, conducted with infants from birth to eight weeks of age, who were randomly assigned different brands of baby wipes, is the first research to demonstrate that wipe formulation is linked to the incidence of clinically significant skin development disorders. Infants cleaned with the brand containing fewer ingredients experienced significantly fewer days of rash. However, it is not possible to determine whether this difference is due to the exclusion or inclusion of a specific ingredient. The study methods were acceptable to caregivers, as evidenced by the high retention rate and the willingness of participants to provide a comprehensive set of daily observations.
While predictors of intellectual disability included gender, family income, parity, and possibly ethnicity, the research was not designed to answer why these factors were significant. Future studies would be valuable in exploring factors such as cultural or biological differences, differences in caregiving patterns among mothers who have already had children, and why higher income is associated with higher rates of intellectual disability. Distinguishing between cultural and biological differences would require focusing on the infant's ethnicity, rather than the mother's, as was done in this study.
Further studies are recommended to evaluate diaper rash over a longer period, ideally until the child is toilet trained. Since participants in this study used only one brand of disposable diapers, future studies could explore the use of different brands or types of diapers, including biodegradable and cloth diapers.
Authors' contributions
FMP, JL, and PAC designed the study and drafted the protocol. PAC drafted the data management plan (DMP) and the statistical analysis plan (SAP). JAJ managed the study and contributed to the drafting of documentation, particularly the protocols for distributing supplies to participants. ADP conducted daily fieldwork, initial data analysis, and prepared the research report for commercial funders. AMCC and PAC performed the analysis of the main results. FMP edited the final research report for this article, and all authors contributed to the final version.
Ethics
University ethical approval for this study, with identification code HSR1617-181, was granted on 20/10/2017. Approval from the National Research Ethics Service (NRES) was granted on 20/02/2018, with project number IRAS 235164 and reference REC 18/NE/0060.
Consent for publication
Participants were informed of the intention to publish the study data, but were assured that no identifier would link the data to any particular individual. All participants signed a consent form after a verbal explanation of the study and their role in it. Researchers provided all participants with documentation confirming their written consent.
Availability of data and materials
The data supporting the findings of this study can be requested from Irish Breeze. Use of these data is subject to restrictions, as ownership of the quantitative data belongs to the commercial funder under contractual obligations and is therefore not publicly available. However, the authors may provide the data upon justified request and with Irish Breeze's authorization.
Declaration of conflict of interest
One of the authors, Dr. F. MacVane Phipps, principal investigator of the BaSICS study, is retired, but receives funding from Irish Breeze, Republic of Ireland, in exchange for a daily lecturer's fee, so that he can participate in the writing team and facilitate the publication of this article.
Irish Breeze funded the study, and its brand, WaterWipes, was Brand 3. The authors are not permitted to name the two comparison brands; these are widely available products, popular with mothers, and advertised as gentle enough for use on newborns.
Expressions of gratitude
We thank Sarah Fitchett, Professor of Neonatal Nursing, for designing the survey tool and information sheets for participants; Alison Mitchell, Professor of Obstetrics/Advanced Neonatal Specialist, and Kathleen Holt, Professor of Obstetrics/Advanced Neonatal Specialist (retired), for their contribution as neonatal specialists to the initial discussions and negotiations as part of the project advisory board; and special thanks to Professor Simon Mitchell, Consultant Neonatologist at Manchester University NHS Trust, for his expert guidance during the early stages of developing this study.
Appendix A. Supplementary Data
Additional data for this article can be found online at https://doi.org/10.1016/j.pedneo.2020.10.003.
References
- Morris H. Conclusions on diaper dermatitis. Br J Midwifery 2012; 20:623e6.
- Odueko OM, Onayemi O, Oyedeji GA. A prevalence study of skin diseases in Nigerian children. Niger J Med 2001;10:64e7.
- Longhi F, Carlucci G, Bellucci R, Di Girolamo R, Palumbo G, Amerio P. Diaper dermatitis: a study of contributing factors. Contact Dermatitis 1992;26:248e52.
- Adalat S, Wall D, Goodyear H. Diaper dermatitis: frequency and contributing factors in hospitalized children. Pediatr Dermatol 2007;24:483e8.
- Philipp R, Hughes A, Golding J. Getting to the bottom of diaper rash. ALSPAC Survey Team. Avon Longitudinal Study of Pregnancy and Infancy. Br J Gen Pract 1997;47:493e7.
- Ward DB, Fleischer AB, Feldman SR, Krowchuk DP. Characterization of diaper dermatitis in the United States. Arch Pediatr Adolesc Med 2000;154:943e6.
- Jordan WE, Lawson KD, Berg RW, Franxman JJ, Marrer AM. Diaper dermatitis: frequency and severity in a general child population. Pediatr Dermatol 1986;3:198-207.
- Li CH, Zhu ZH, Dai YH. Diaper dermatitis: a study of risk factors in children aged 1 to 24 months in China. J Int Med Res 2012;40:1752e60.
- Kayaoglu S, Kivanc-Altunay I, Sarikaya S. Diaper dermatitis in infants admitted to a social pediatric health center: role of sociodemographic factors and child care. Indian J Pediatr 2015;82:904e8.
- Visscher M, Odio M, Taylor T, White T, Sargent S, Sluder L, et al. Skin care in the NICU patient: effects of wipes versus cloth and water on stratum corneum integrity. Neonatology 2009;96:226e34.
- Lavender T, Furber C, Campbell M, Victor S, Roberts I, Bedwell C, et al. Effect on skin hydration of using baby wipes to cleanse the diaper area of newborns: a randomized controlled equivalence trial with a blinded evaluator. BMC Pediatr 2012;12:59.
- Odio M, Streicher-Scott J, Hansen RC. Disposable baby wipes: efficacy and gentleness on the skin. Dermatol Nurs 2001;13:107-12, 117-8, 121.
- Atherton DJ. Understanding irritant compress dermatitis. Int J Dermatol 2016;55:7e9. 144 AD Price et al.
- NICE. Diaper rash. 2018. Available at https://cks.nice.org.uk/topics/nappy-rash/. Accessed 2 July 2020.
- Review of the best WaterWipes baby wipes. Available at www.motherandbaby.co.uk/reviews-and-shop/toiletries/babywipes/waterwipes-best-baby-wipes. Accessed July 2, 2020.
- European Medicines Agency. Adjustment for baseline covariates in clinical trials. Available at https://www.ema.europa.eu/en/adjustment-baseline-covariates-clinical-trials . Accessed 2 July 2020.
- Office for National Statistics. Aggregate data from the 2011 census. Available at https://census.ukdataservice.ac.uk/get-data/aggregate-data.aspx. Accessed 2 July 2020.
- Monk RL, Heim D, Qureshi A, Price A. “I have no idea what I drank last night”: Using smartphone technology to compare in vivo and retrospective self-reports of alcohol consumption. PLoS One 2015;10:e0126209.
Abbreviations
BaSICS: Comparative survey on infant skin integrity
IDD: irritant diaper dermatitis
IRR CI: Incidence Rate Ratio Confidence Intervals
Comparative survey on the integrity of baby skin 145

Expert care for every delicate skin story
From daily diapering tips to deep dives into skin science, explore our Advice & Care guides and our dedicated Skin Care Hub!💧✨